Neck Cancer Symtoms
Source(google.com.pk)
1.What are cancers of the head and neck?
Cancers that are known collectively as head and neck cancers usually begin in the squamous cells that line the moist, mucosal surfaces inside the head and neck (for example, inside the mouth, the nose, and the throat). These squamous cell cancers are often referred to as squamous cell carcinomas of the head and neck. Head and neck cancers can also begin in the salivary glands, but salivary gland cancers are relatively uncommon. Salivary glands contain many different types of cells that can become cancerous, so there are many different types of salivary gland cancer.
Cancers of the head and neck are further categorized by the area of the head or neck in which they begin. These areas are described below and labeled in the image of head and neck cancer regions.
Oral cavity: Includes the lips, the front two-thirds of the tongue, the gums, the lining inside the cheeks and lips, the floor (bottom) of the mouth under the tongue, the hard palate (bony top of the mouth), and the small area of the gum behind the wisdom teeth.
Pharynx: The pharynx (throat) is a hollow tube about 5 inches long that starts behind the nose and leads to the esophagus. It has three parts: the nasopharynx (the upper part of the pharynx, behind the nose); the oropharynx (the middle part of the pharynx, including the soft palate [the back of the mouth], the base of the tongue, and the tonsils); the hypopharynx (the lower part of the pharynx).
Larynx: The larynx, also called the voicebox, is a short passageway formed by cartilage just below the pharynx in the neck. The larynx contains the vocal cords. It also has a small piece of tissue, called the epiglottis, which moves to cover the larynx to prevent food from entering the air passages.
Paranasal sinuses and nasal cavity: The paranasal sinuses are small hollow spaces in the bones of the head surrounding the nose. The nasal cavity is the hollow space inside the nose.
Salivary glands: The major salivary glands are in the floor of the mouth and near the jawbone. The salivary glands produce saliva.
Head and neck cancer regions. Illustrates location of paranasal sinuses, nasal cavity, oral cavity, tongue, salivary glands, larynx, and pharynx (including the nasopharynx, oropharynx, and hypopharynx).
Cancers of the brain, the eye, the esophagus, and the thyroid gland, as well as those of the scalp, skin, muscles, and bones of the head and neck, are not usually classified as head and neck cancers.
Sometimes, cancerous squamous cells can be found in the lymph nodes of the upper neck when there is no evidence of cancer in other parts of the head and neck (1). When this happens, the cancer is called metastatic squamous neck cancer with unknown (occult) primary. More information about this cancer type can be found in Metastatic Squamous Neck Cancer with Occult Primary (PDQ®).
2.What causes cancers of the head and neck?
Alcohol and tobacco use (including smokeless tobacco, sometimes called “chewing tobacco” or “snuff”) are the two most important risk factors for head and neck cancers, especially cancers of the oral cavity, oropharynx, hypopharynx, and larynx (2–5). At least 75 percent of head and neck cancers are caused by tobacco and alcohol use (6). People who use both tobacco and alcohol are at greater risk of developing these cancers than people who use either tobacco or alcohol alone (6–8). Tobacco and alcohol use are not risk factors for salivary gland cancers.
Infection with cancer-causing types of human papillomavirus (HPV), especially HPV-16, is a risk factor for some types of head and neck cancers, particularly oropharyngeal cancers that involve the tonsils or the base of the tongue (9–11). In the United States, the incidence of oropharyngeal cancers caused by HPV infection is increasing, while the incidence of oropharyngeal cancers related to other causes is falling (9). More information is available in the HPV and Cancer fact sheet.
Other risk factors for cancers of the head and neck include the following:
Paan (betel quid). Immigrants from Southeast Asia who use paan (betel quid) in the mouth should be aware that this habit has been strongly associated with an increased risk of oral cancer (12, 13).
Maté. Consumption of maté, a tea-like beverage habitually consumed by South Americans, has been associated with an increased risk of cancers of the mouth, throat, esophagus, and larynx (13, 14).
Preserved or salted foods. Consumption of certain preserved or salted foods during childhood is a risk factor for nasopharyngeal cancer (15, 16).
Oral health. Poor oral hygiene and missing teeth may be weak risk factors for cancers of the oral cavity (17, 18). Use of mouthwash that has a high alcohol content is a possible, but not proven, risk factor for cancers of the oral cavity (17, 18).
Occupational exposure. Occupational exposure to wood dust is a risk factor for nasopharyngeal cancer (15, 16). Certain industrial exposures, including exposures to asbestos and synthetic fibers, have been associated with cancer of the larynx, but the increase in risk remains controversial (19). People working in certain jobs in the construction, metal, textile, ceramic, logging, and food industries may have an increased risk of cancer of the larynx (20). Industrial exposure to wood or nickel dust or formaldehyde is a risk factor for cancers of the paranasal sinuses and nasal cavity (21–23).
Radiation exposure. Radiation to the head and neck, for noncancerous conditions or cancer, is a risk factor for cancer of the salivary glands (17, 24, 25).
Epstein-Barr virus infection. Infection with the Epstein-Barr virus is a risk factor for nasopharyngeal cancer (26) and cancer of the salivary glands (27, 28).
Ancestry. Asian ancestry, particularly Chinese ancestry, is a risk factor for nasopharyngeal cancer (15, 16).
3.What are the symptoms of head and neck cancers?
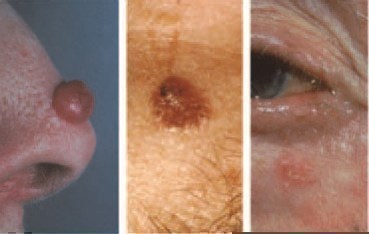
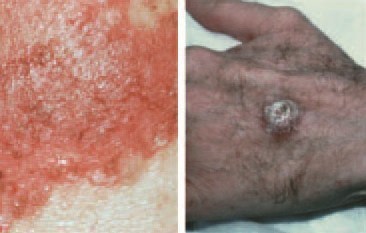
The symptoms of head and neck cancers may include a lump or a sore that does not heal, a sore throat that does not go away, difficulty in swallowing, and a change or hoarseness in the voice. These symptoms may also be caused by other, less serious conditions. It is important to check with a doctor or dentist about any of these symptoms. Symptoms that may affect specific areas of the head and neck include the following:
Oral cavity. A white or red patch on the gums, the tongue, or the lining of the mouth; a swelling of the jaw that causes dentures to fit poorly or become uncomfortable; and unusual bleeding or pain in the mouth.
Pharynx. Trouble breathing or speaking; pain when swallowing; pain in the neck or the throat that does not go away; frequent headaches, pain, or ringing in the ears; or trouble hearing.
Larynx. Pain when swallowing or ear pain.
Paranasal sinuses and nasal cavity. Sinuses that are blocked and do not clear; chronic sinus infections that do not respond to treatment with antibiotics; bleeding through the nose; frequent headaches, swelling or other trouble with the eyes; pain in the upper teeth; or problems with dentures.
Salivary glands. Swelling under the chin or around the jawbone, numbness or paralysis of the muscles in the face, or pain in the face, the chin, or the neck that does not go away.
4.How common are head and neck cancers?
Head and neck cancers account for approximately 3 percent of all cancers in the United States (29). These cancers are nearly twice as common among men as they are among women (30). Head and neck cancers are also diagnosed more often among people over age 50 than they are among younger people.
Researchers estimated that more than 52,000 men and women in this country would be diagnosed with head and neck cancers in 2012 (30).
5.How can I reduce my risk of developing head and neck cancers?
People who are at risk of head and neck cancers―particularly those who use tobacco―should talk with their doctor about ways that they may be able to reduce their risk. They should also discuss with their doctor how often to have checkups. In addition, ongoing clinical trials are testing the effectiveness of various medications in preventing head and neck cancers in people who have a high risk of developing these diseases. A list of these trials can be found at the link below.
Clinical Trials To Prevent Head and Neck Cancers
Information specialists from NCI’s Cancer Information Service (CIS) can also help people find clinical trials for the prevention of head and neck cancers. The CIS can be reached at 1–800–4–CANCER (1–800–422–6237) or by chatting with a cancer information specialist online through LiveHelp.
Avoiding oral HPV infection may reduce the risk of HPV-associated head and neck cancers. However, it is not yet known whether the Food and Drug Administration-approved HPV vaccines Gardasil® and Cervarix® prevent HPV infection of the oral cavity, and neither vaccine has yet been approved for the prevention of oropharyngeal cancer. More information about these vaccines is in the NCI fact sheet Human Papillomavirus (HPV) Vaccines.
6.How are head and neck cancers diagnosed?
To find the cause of the signs or symptoms of a problem in the head and neck area, a doctor evaluates a person’s medical history, performs a physical examination, and orders diagnostic tests. The exams and tests may vary depending on the symptoms. Examination of a sample of tissue under a microscope is always necessary to confirm a diagnosis of cancer.
More information about the specific tests and procedures used to diagnose cancer is available in What You Need To Know About™ Cancer: Diagnosis.
If the diagnosis is cancer, the doctor will want to learn the stage (or extent) of disease. Staging is a careful attempt to find out whether the cancer has spread and, if so, to which parts of the body. Staging may involve an examination under anesthesia (in an operating room), x-rays and other imaging procedures, and laboratory tests. Knowing the stage of the disease helps the doctor plan treatment.
7.How are head and neck cancers treated?
The treatment plan for an individual patient depends on a number of factors, including the exact location of the tumor, the stage of the cancer, and the person’s age and general health. Treatment for head and neck cancer can include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of treatments. General information about treatment options for cancer is available in What You Need To Know About™ Cancer: Treatment.
People who are diagnosed with HPV-positive oropharyngeal cancer may be treated differently than people with oropharyngeal cancers that are HPV-negative. Recent research has shown that patients with HPV-positive oropharyngeal tumors have a better prognosis and may do just as well on less intense treatment. An ongoing clinical trial is investigating this question.
More information about treatment for specific types of head and neck cancers is in the following PDQ® cancer treatment summaries, which are available in patient and health professional versions, as well as in Spanish (the links below go to the patient versions in English):
Hypopharyngeal Cancer
Laryngeal Cancer
Lip and Oral Cavity Cancer
Metastatic Squamous Neck Cancer with Occult Primary
Nasopharyngeal Cancer
Oropharyngeal Cancer
Paranasal Sinus and Nasal Cavity Cancer
Salivary Gland Cancer
The patient and the doctor should consider treatment options carefully. They should discuss each type of treatment and how it might change the way the patient looks, talks, eats, or breathes.
8.What are the side effects of treatment?
Surgery for head and neck cancers often changes the patient’s ability to chew, swallow, or talk. The patient may look different after surgery, and the face and neck may be swollen. The swelling usually goes away within a few weeks. However, if lymph nodes are removed, the flow of lymph in the area where they were removed may be slower and lymph could collect in the tissues, causing additional swelling; this swelling may last for a long time.
After a laryngectomy (surgery to remove the larynx) or other surgery in the neck, parts of the neck and throat may feel numb because nerves have been cut. If lymph nodes in the neck were removed, the shoulder and neck may become weak and stiff.
Patients who receive radiation to the head and neck may experience redness, irritation, and sores in the mouth; a dry mouth or thickened saliva; difficulty in swallowing; changes in taste; or nausea. Other problems that may occur during treatment are loss of taste, which may decrease appetite and affect nutrition, and earaches (caused by the hardening of ear wax). Patients may also notice some swelling or drooping of the skin under the chin and changes in the texture of the skin. The jaw may feel stiff, and patients may not be able to open their mouth as wide as before treatment.
Patients should report any side effects to their doctor or nurse, and discuss how to deal with them. Information about rehabilitation after surgery for head and neck cancer can be found in the answer to Question 10.
Where can I find more information about clinical trials for patients with head and neck cancers?
Clinical trials are research studies conducted with people who volunteer to take part. Participation in clinical trials is an option for many patients with head and neck cancer. A list of clinical trials to treat head and neck cancers can be found at the link below.
Clinical Trials To Treat Head and Neck Cancers
People interested in taking part in a clinical trial should talk with their doctor. Information about clinical trials is available in the NCI booklet Taking Part in Cancer Treatment Research Studies. This booklet describes how research studies are carried out and explains their possible benefits and risks.
NCI provides information about specific clinical trials for people who have head and neck cancers. Questions about these trials can be answered by NCI’s Cancer Information Service at 1–800–4–CANCER (1–800–422–6237), or by chatting with a cancer information specialist online through LiveHelp.
What rehabilitation or support options are available for patients with head and neck cancers?
The goal of treatment for head and neck cancers is to control the disease, but doctors are also concerned about preserving the function of the affected areas as much as they can and helping the patient return to normal activities as soon as possible after treatment. Rehabilitation is a very important part of this process. The goals of rehabilitation depend on the extent of the disease and the treatment that a patient has received.
Depending on the location of the cancer and the type of treatment, rehabilitation may include physical therapy, dietary counseling, speech therapy, and/or learning how to care for a stoma. A stoma is an opening into the windpipe through which a patient breathes after a laryngectomy, which is surgery to remove the larynx. The National Library of Medicine has more information about laryngectomy in MedlinePlus.
Sometimes, especially with cancer of the oral cavity, a patient may need reconstructive and plastic surgery to rebuild bones or tissues. However, reconstructive surgery may not always be possible because of damage to the remaining tissue from the original surgery or from radiation therapy. If reconstructive surgery is not possible, a prosthodontist may be able to make a prosthesis (an artificial dental and/or facial part) to restore satisfactory swallowing, speech, and appearance. Patients will receive special training on how to use the device.
Patients who have trouble speaking after treatment may need speech therapy. Often, a speech-language pathologist will visit the patient in the hospital to plan therapy and teach speech exercises or alternative methods of speaking. Speech therapy usually continues after the patient returns home.
Eating may be difficult after treatment for head and neck cancer. Some patients receive nutrients directly into a vein after surgery or need a feeding tube until they can eat on their own. A feeding tube is a flexible plastic tube that is passed into the stomach through the nose or an incision in the abdomen. A nurse or speech-language pathologist can help patients learn how to swallow again after surgery. The NCI booklet Eating Hints: Before, During, and After Cancer Treatment contains many useful suggestions and recipes.
9.Is follow-up care necessary? What does it involve?
Regular follow-up care is very important after treatment for head and neck cancer to make sure that the cancer has not returned, or that a second primary (new) cancer has not developed. Depending on the type of cancer, medical checkups could include exams of the stoma, if one has been created, and of the mouth, neck, and throat. Regular dental exams may also be necessary.
From time to time, the doctor may perform a complete physical exam, blood tests, x-rays, and computed tomography (CT), positron emission tomography (PET), or magnetic resonance imaging (MRI) scans. The doctor may monitor thyroid and pituitary gland function, especially if the head or neck was treated with radiation. Also, the doctor is likely to counsel patients to stop smoking. Research has shown that continued smoking by a patient with head and neck cancer may reduce the effectiveness of treatment and increase the chance of a second primary cancer (see Question 12).
Additional information can be found in the NCI fact sheet Follow-up Care After Cancer Treatment.
10.How can people who have had head and neck cancers reduce their risk of developing a second primary (new) cancer?
People who have been treated for head and neck cancers have an increased chance of developing a new cancer, usually in the head, neck, esophagus, or lungs (31–33). The chance of a second primary cancer varies depending on the site of the original cancer, but it is higher for people who use tobacco and drink alcohol (31).
Especially because patients who smoke have a higher risk of a second primary cancer, doctors encourage patients who use tobacco to quit. Information about tobacco cessation is available from NCI’s Cancer Information Service at 1–800–4–CANCER (1–800–422–6237) and in the NCI fact sheet Where To Get Help When You Decide To Quit Smoking. The federal government’s main resource to help people quit using tobacco is BeTobaccoFree.gov.The government also sponsors Smokefree Women, a website to help women quit using tobacco, and Smokefree Teen, which is designed to help teens understand the decisions they make and how those decisions fit into their lives. The toll-free number 1–800–QUIT–NOW (1–800–784–8669) also serves as a single point of access to state-based telephone quitlines.
Selected References
Mendenhall WM, Mancuso AA, Amdur RJ, et al. Squamous cell carcinoma metastatic to the neck from an unknown head and neck primary site. American Journal of Otolaryngology 2001; 22(4):281–287. [PubMed Abstract]
Gandini S, Botteri E, Iodice S, et al. Tobacco smoking and cancer: a meta-analysis. International Journal of Cancer 2008; 122(1):155–164. [PubMed Abstract]
Hashibe M, Boffetta P, Zaridze D, et al. Evidence for an important role of alcohol- and aldehyde-metabolizing genes in cancers of the upper aerodigestive tract. Cancer Epidemiology, Biomarkers and Prevention 2006; 15(4):696–703. [PubMed Abstract]
Hashibe M, Brennan P, Benhamou S, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Journal of the National Cancer Institute 2007; 99(10):777–789. [PubMed Abstract]
Boffetta P, Hecht S, Gray N, Gupta P, Straif K. Smokeless tobacco and cancer. The Lancet Oncology 2008; 9(7):667–675. [PubMed Abstract]
Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Research 1988; 48(11):3282–3287. [PubMed Abstract]
Tuyns AJ, Estève J, Raymond L, et al. Cancer of the larynx/hypopharynx, tobacco and alcohol: IARC international case-control study in Turin and Varese (Italy), Zaragoza and Navarra (Spain), Geneva (Switzerland) and Calvados (France). International Journal of Cancer 1988; 41(4):483–491. [PubMed Abstract]
Hashibe M, Brennan P, Chuang SC, et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiology, Biomarkers and Prevention 2009; 18(2):541–550. [PubMed Abstract]
Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. Journal of Clinical Oncology 2011; 29(32):4294–4301. [PubMed Abstract]
Adelstein DJ, Ridge JA, Gillison ML, et al. Head and neck squamous cell cancer and the human papillomavirus: summary of a National Cancer Institute State of the Science Meeting, November 9–10, 2008, Washington, D.C. Head and Neck 2009; 31(11):1393–1422. [PubMed Abstract]
Gillison ML, D’Souza G, Westra W, et al. Distinct risk factors profiles for human papillomavirus type 16-positive and human papillomavirus type-16 negative head and neck cancers. Journal of the National Cancer Institute 2008; 100(6):407–420. [PubMed Abstract]
Ho PS, Ko YC, Yang YH, Shieh TY, Tsai CC. The incidence of oropharyngeal cancer in Taiwan: an endemic betel quid chewing area. Journal of Oral Pathology and Medicine 2002; 31(4):213–219. [PubMed Abstract]
Goldenberg D, Lee J, Koch WM, et al. Habitual risk factors for head and neck cancer. Otolaryngology and Head and Neck Surgery 2004; 131(6):986–993. [PubMed Abstract]
Goldenberg D, Golz A, Joachims HZ. The beverage maté: a risk factor for cancer of the head and neck. Head and Neck 2003; 25(7):595–601. [PubMed Abstract]
Yu MC, Yuan JM. Nasopharyngeal Cancer. In: Schottenfeld D, Fraumeni JF Jr., editors. Cancer Epidemiology and Prevention. 3rd ed. New York: Oxford University Press, 2006.
Yu MC, Yuan JM. Epidemiology of nasopharyngeal carcinoma. Seminars in Cancer Biology 2002; 12(6):421–429. [PubMed Abstract]
Mayne ST, Morse DE, Winn DM. Cancers of the Oral Cavity and Pharynx. In: Schottenfeld D, Fraumeni JF Jr., editors. Cancer Epidemiology and Prevention. 3rd ed. New York: Oxford University Press, 2006.
Guha N, Boffetta P, Wünsch Filho V, et al. Oral health and risk of squamous cell carcinoma of the head and neck and esophagus: results of two multicentric case-control studies. American Journal of Epidemiology 2007; 166(10):1159–1173. [PubMed Abstract]
Olshan AF. Cancer of the Larynx. In: Schottenfeld D, Fraumeni JF Jr., editors. Cancer Epidemiology and Prevention. 3rd ed. New York: Oxford University Press, 2006.
Boffetta P, Richiardi L, Berrino F, et al. Occupation and larynx and hypopharynx cancer: an international case-control study in France, Italy, Spain, and Switzerland. Cancer Causes and Control 2003; 14(3):203–212. [PubMed Abstract]
Littman AJ, Vaughan TL. Cancers of the Nasal Cavity and Paranasal Sinuses. In: Schottenfeld D, Fraumeni JF Jr., editors. Cancer Epidemiology and Prevention. 3rd ed. New York: Oxford University Press, 2006.
Luce D, Leclerc A, Bégin D, et al. Sinonasal cancer and occupational exposures: a pooled analysis of 12 case-control studies. Cancer Causes and Control 2002; 13(2):147–157. [PubMed Abstract]
Luce D, Gérin M, Leclerc A, et al. Sinonasal cancer and occupational exposure to formaldehyde and other substances. International Journal of Cancer 1993; 53(2):224–231. [PubMed Abstract]
Preston-Martin S, Thomas DC, White SC, Cohen D. Prior exposure to medical and dental x-rays related to tumors of the parotid gland. Journal of the National Cancer Institute 1988; 80(12):943–949. [PubMed Abstract]
Horn-Ross PL, Ljung BM, Morrow M. Environmental factors and the risk of salivary gland cancer. Epidemiology 1997; 8(4):414–429. [PubMed Abstract]
Chien YC, Chen JY, Liu MY, et al. Serologic markers of Epstein-Barr virus infection and nasopharyngeal carcinoma in Taiwanese men. New England Journal of Medicine 2001; 345(26):1877–1882. [PubMed Abstract]
Hamilton-Dutoit SJ, Therkildsen MH, Neilsen NH, et al. Undifferentiated carcinoma of the salivary gland in Greenlandic Eskimos: demonstration of Epstein-Barr virus DNA by in situ nucleic acid hybridization. Human Pathology 1991; 22(8):811–815. [PubMed Abstract]
Chan JK, Yip TT, Tsang WY, et al. Specific association of Epstein-Barr virus with lymphoepithelial carcinoma among tumors and tumorlike lesions of the salivary gland. Archives of Pathology and Laboratory Medicine 1994; 118(10):994–997. [PubMed Abstract]
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA: A Cancer Journal for Clinicians 2010; 60(5):277–300. [PubMed Abstract]
American Cancer Society (2012). Cancer Facts and Figures 2012 Exit Disclaimer. Atlanta, GA: American Cancer Society. Retrieved December 26, 2012.
Do KA, Johnson MM, Doherty DA, et al. Second primary tumors in patients with upper aerodigestive tract cancers: joint effects of smoking and alcohol (United States). Cancer Causes and Control 2003; 14(2):131–138. [PubMed Abstract]
Argiris A, Brockstein BE, Haraf DJ, et al. Competing causes of death and second primary tumors in patients with locoregionally advanced head and neck cancer treated with chemoradiotherapy. Clinical Cancer Research 2004; 10(6)1956–1962. [PubMed Abstract]
Chuang SC, Scelo G, Tonita JM, et al. Risk of second primary cancer among patients with head and neck cancers: a pooled analysis of 13 cancer registries. International Journal of Cancer 2008; 123(10):2390–2396. [PubMed Abstract]